
The TNM staging system for prostate cancer describes how far the tumour has grown, whether it has reached nearby lymph nodes, and whether it has spread to other organs. Each letter gives your medical team a specific piece of information that shapes your diagnosis and treatment plan.


The TNM staging system for prostate cancer is the tool doctors use to describe how far the cancer has grown, where it sits, and whether it has moved anywhere else in the body. If you have just received a staging result and the letters and numbers feel meaningless right now, you are not the only one to find them baffling.
Most people leave the clinic with a sheet of paper that says something like “T2c N0 M0” and have no idea what any of it tells them about their life going forward. This guide explains it properly, not in clinical shorthand, but in real terms, so you understand what each part of your stage says, how doctors work it out, and what it signals about your treatment options.
Prostate cancer is now the most commonly diagnosed cancer in the UK, with more than 64,000 men diagnosed every year. And around 8 in 10 men in the UK survive prostate cancer for ten years or more. Staging plays a big part in making those outcomes possible because it tells the team exactly what they are dealing with and how to treat it.
What the TNM staging system for prostate cancer is
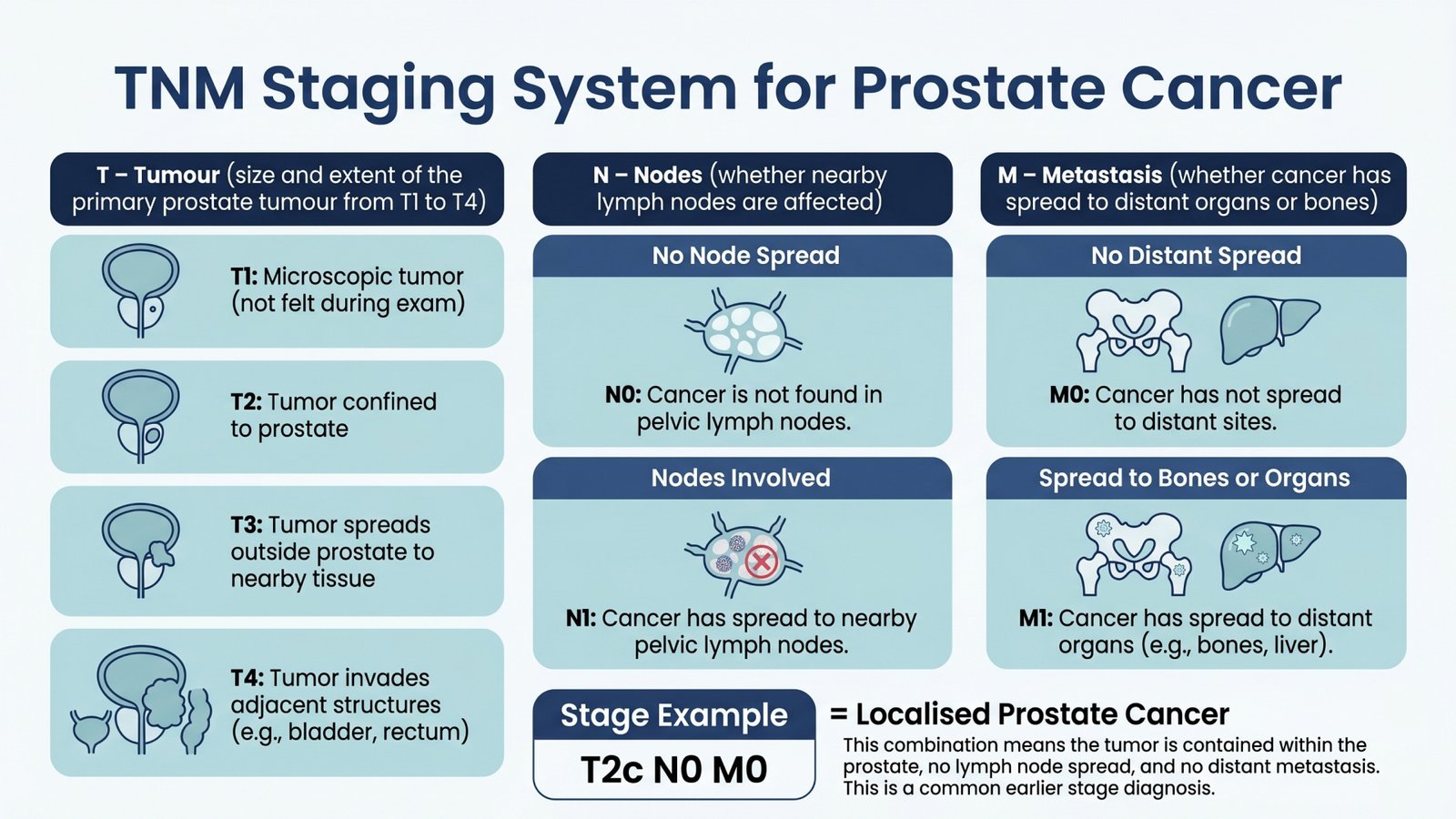
TNM stands for Tumour, Node, Metastasis. Each letter describes one dimension of the cancer, and doctors assess each one separately before putting them together into a full picture.
Think of it as three separate questions your medical team works through:
- How big is the tumour and has it grown beyond the prostate?
- Has it reached the nearby lymph nodes?
- Has it spread to other organs or bones?
The answers, combined with your PSA blood test result and Grade Group (a measure of how aggressive the cancer cells look under a microscope), give doctors your full stage from Stage I to Stage IV.
There are also two versions of the T part of the system worth knowing about upfront.
The clinical T stage (written as cT) is what doctors work out before any surgery, using a physical examination, biopsy, blood tests, and MRI scans.
The pathological T stage (written as pT) only becomes available after surgery, when a pathologist examines the removed prostate in the lab. Pathological staging tends to be more accurate because the full tissue is right there to look at, but it only applies to men who have the prostate surgically removed.
The T category: where is the tumour and how far has it grown?
The T in TNM describes the primary tumour, which is the original cancer site in the prostate. It ranges from T1 (the smallest and most contained) to T4 (the most locally advanced), and each level tells your doctors something specific about where the cancer sits and how far it has travelled within or beyond the prostate gland.
T1: the cancer is there, but cannot be felt or seen
At T1, the tumour is too small to be felt during a physical examination and does not show up on a routine scan. It is only found because something else prompted a test.
T1 has three subcategories:
- T1a: Cancer was found in 5% or less of tissue removed during a procedure for an enlarged prostate, called a TURP (transurethral resection of the prostate). Nobody was looking for cancer. It was picked up by accident.
- T1b: Same situation as T1a, but cancer was found in more than 5% of the removed tissue.
- T1c: Cancer was found through a targeted biopsy done specifically because the PSA blood test came back high, even though nothing could be felt during examination. This is the most common scenario in current practice.
For many men with T1 disease, the first recommendation is active surveillance rather than immediate treatment. Active surveillance does not mean being sent home and forgotten. It means regular PSA tests, periodic biopsies, and imaging to keep a close eye on the cancer over time.
If it starts growing, treatment begins then. For slow-moving T1 cancers, starting treatment straight away can sometimes cause more harm than the cancer itself would over the same period.
T2: the cancer is bigger, but still inside the prostate
At T2, the tumour has grown larger and may be detectable during a physical exam or on an MRI scan. But it has not broken through the outer layer of the prostate (the capsule), so it is still contained within the gland.
T2 has three subcategories:
- T2a: Cancer is in no more than half of one side of the prostate.
- T2b: Cancer is in more than half of one side but has not crossed to the other side.
- T2c: Cancer is present in both sides of the prostate.
T2 is still described as localised prostate cancer, which means it has not spread beyond the prostate. Men at this stage are generally offered curative treatment options, including surgery to remove the prostate, external beam radiotherapy, or brachytherapy (where radioactive seeds or wires deliver radiation directly inside the prostate).
One important detail is that around 15 to 35% of men staged as T2 before surgery are found to have T3 disease once the removed prostate is examined in the lab. This is not a mistake in the original staging. It happens because imaging cannot always pick up tiny amounts of spread beyond the capsule.
T3: the cancer has broken through the outer wall of the prostate
At T3, the cancer has grown through the capsule surrounding the prostate. This is called locally advanced prostate cancer, which means the tumour is no longer fully contained inside the gland.
T3 has two subcategories:
- T3a: The cancer has pushed through the capsule but has not yet reached the seminal vesicles. The seminal vesicles are two small pouches that sit just behind the prostate and produce the fluid that carries sperm. Doctors call this spread extraprostatic extension.
- T3b: The cancer has spread into the seminal vesicles.
Treatment at T3 is more intensive than at T1 or T2. Radiotherapy is commonly paired with hormone therapy, also called androgen deprivation therapy (ADT). This combination is well-evidenced to be more effective than radiotherapy alone for locally advanced disease.
Hormone therapy at this stage typically runs for 18 to 36 months, depending on other risk factors. Surgery is still an option for some men with T3a disease, particularly those who are fit and for whom the cancer has not spread too widely beyond the capsule. Post-operative radiotherapy is often needed as a follow-up in these cases.
T4: the cancer has grown into nearby structures
At T4, the tumour has extended into structures beyond the prostate and its immediate surroundings. These structures can include:
- the urethral sphincter (the muscle that controls urine flow)
- the rectum
- the bladder
- the wall of the pelvis
Treatment at T4 depends heavily on whether the cancer has also spread to lymph nodes or distant organs. For T4 disease without distant spread, external beam radiotherapy combined with long-term hormone therapy is the standard approach. Surgery becomes technically difficult at this stage and is only considered at specialist centres for carefully selected men.
The N category: has cancer reached the nearby lymph nodes?
Lymph nodes are small, bean-shaped structures throughout the body that form part of the immune system. The ones near the prostate sit in the pelvis, and they can be one of the first places prostate cancer travels to beyond the gland. The N category tells doctors whether any of those nodes contain cancer cells.
There are three possible N results:
- NX: The lymph nodes were not assessed. This happens when no lymph node removal took place as part of the diagnostic workup.
- N0: No cancer was found in the nearby lymph nodes.
- N1: Cancer cells were found in one or more nearby lymph nodes.
N1 is a significant finding. It tells your team that cancer has started moving beyond the prostate into the surrounding lymphatic system, even if it has not reached distant organs yet. For most men with N1 disease, the standard approach is radiotherapy combined with long-term hormone therapy.
Lymph nodes are assessed either through MRI or CT imaging before treatment, or by removing and examining them surgically during a prostatectomy. Small deposits of cancer in lymph nodes can be missed on imaging. This is another reason why pathological staging after surgery can sometimes reveal N1 disease that was not picked up beforehand.
The M category: has the cancer spread to other parts of the body?
The M in the TNM staging system for prostate cancer stands for metastasis, which simply means spread. It describes whether cancer has moved beyond the prostate and nearby lymph nodes to other parts of the body entirely.
There are two main results here. M0 tells you no distant spread has been detected. M1 tells you the cancer has spread, and it is broken down further based on where:
- M1a: Cancer has moved to distant lymph nodes, specifically those outside the pelvic area.
- M1b: Cancer has spread to the bone. This is the most common site prostate cancer travels to. It does not mean the cancer started in the bone. It means prostate cancer cells have travelled there through the bloodstream.
- M1c: Cancer has spread to other organs such as the liver, lungs, or brain.
When spread is present in more than one site, the most advanced category is the one used for staging.
For men with metastatic prostate cancer, treatment shifts to managing the disease across the whole body rather than targeting the prostate alone. Hormone therapy is the core treatment at this stage, often combined with chemotherapy or newer hormonal medicines, depending on the individual situation.
Not all men with bone spread feel pain straight away. Bone metastases are usually found through a bone scan or a PSMA-PET scan, which is a more sensitive type of imaging now increasingly available in the UK. For more on day-to-day life after a metastatic diagnosis, the guide on living with metastatic prostate cancer covers what to expect practically.
How PSA and Grade Group complete the staging picture
The TNM staging system for prostate cancer gives the anatomical picture, but two other results fill in the biological side of things. Together, all three create a much more accurate picture of the cancer than any one result on its own.
PSA is a protein made by prostate cells and measured through a simple blood test. A higher PSA at diagnosis generally points to more active disease, and a PSA above 20 ng/mL is typically associated with higher-risk prostate cancer. This affects decisions about whether additional treatment is needed on top of surgery or radiotherapy.
Grade Group is based on the Gleason score, which comes from looking at biopsy tissue under a microscope. Here is how it works:
- A pathologist looks at the two most common patterns of cancer cells found in the biopsy sample.
- Each pattern gets scored from 1 to 5 based on how abnormal the cells look.
- Those two scores are added together to give the Gleason score, which runs from 6 to 10.
- That Gleason score then maps to a Grade Group from 1 to 5, where Grade Group 1 is the least aggressive, and Grade Group 5 is the most.
When TNM, PSA, and Grade Group are combined, doctors assign the overall stage from Stage I to Stage IV. In the UK, the Cambridge Prognostic Group (CPG) system is also used for localised disease. It places patients into five risk groups based on Grade Group, PSA, and T stage, giving a more detailed picture for men whose disease falls somewhere in the middle ground.
How staging connects to treatment
Each stage points toward a different treatment pathway. Here is how the two connect:
- Stage I (T1, N0, M0, low Grade Group, low PSA): Active surveillance is the usual starting point. Many men at this stage never need treatment.
- Stage II (T1 to T2, N0, M0): Curative treatment is offered, including surgery, radiotherapy, or brachytherapy. Active surveillance remains an option for lower-risk cases.
- Stage III (T3 to T4, N0, M0): Radiotherapy combined with hormone therapy is standard for locally advanced disease. Surgery is possible in selected T3a cases.
- Stage IV (any T with N1 or M1): Systemic treatment leads the way. Hormone therapy is the backbone, often combined with chemotherapy or newer hormonal agents for M1 disease.
Your stage is a starting point, not an ending
Getting a staging result can feel like a door closing. In reality, it is the point where your clinical team gets the clearest picture of what they are working with and how to approach it.
The TNM staging system for prostate cancer exists to bring structure to a complicated situation. It gives your doctors a shared language to plan treatment, track progress, and make decisions that are specific to you rather than generic.
If you have questions about your staging result or want to understand your treatment options in more detail, Dr Carla Perna and the team are here to help. Book a consultation and get the clarity you need to move forward with confidence.
Frequently asked questions
What does T2c N0 M0 tell you in plain terms?
It tells you the cancer is present in both sides of the prostate but has not broken through the oute. wall of the gland. It has not reached any nearby lymph nodes and has not spread to distant organs. This is localised prostate cancer, and curative treatment options are available.
Can your stage change after treatment starts?
Your formal stage does not change. But the pathological stage assigned after surgery can differ from the clinical stage given before it. A pre-surgery T2 can become a post-surgery T3 once the full prostate is examined in the lab, and this can affect whether additional treatment like post-operative radiotherapy is recommended.
Does Stage IV always point to a cancer that cannot be treated?
No. Stage IV includes men with N1 disease (spread to nearby pelvic lymph nodes only) and men with distant metastases. For men with N1 disease and no distant spread, long-term disease control is genuinely achievable. For men with M1 disease, treatment focuses on controlling the cancer and maintaining quality of life, and many men live well for years with the right management in place.
How do doctors check lymph nodes without surgery?
Lymph node status is assessed through imaging, typically MRI or CT scans. However, imaging cannot always detect tiny deposits of cancer in nodes that appear normal in size. PSMA-PET CT scans, which are increasingly available in the UK, are more sensitive and can detect spread that conventional imaging misses.
Does a high PSA automatically point to a higher stage?
Not always. Some men have high PSA levels with cancer that is still contained in the prostate. Some men with locally advanced disease have relatively low PSA levels. PSA is one part of the staging picture, and on its own, it does not determine your stage. The T, N, and M categories and the Grade Group all feed into the final assessment together.
What is the difference between clinical and pathological staging?
Clinical staging is assessed before any surgery, using examination findings, PSA, biopsy results, and imaging. Pathological staging happens after the prostate is surgically removed and examined in a laboratory. Pathological staging is more accurate because the whole specimen can be assessed directly. For men who have radiotherapy instead of surgery, pathological staging is not possible, so clinical staging remains the basis for all decisions throughout their care.



